Demand changes. Service expectations rise. Technology footprints expand. The pressure to respond faster becomes constant. Most of the time, when an organisation decides to change how it operates, the consequences of getting it wrong are commercial. Missed targets. Delayed timelines. A dent in quarterly performance. Painful, but recoverable.
Then there are the rarer engagements, where the stakes sit at a completely different level. Where the technology environment being transformed is the operational backbone of a public health system. Where the applications being managed are not productivity tools or internal business platforms, but the digital infrastructure keeping hospitals running, surgical theatres functioning, emergency departments responsive, and clinical staff connected across one of the most geographically demanding service environments in the world.
When Citrus Global, our subsidiary, took on this engagement, they stepped into exactly that environment.
The Environment
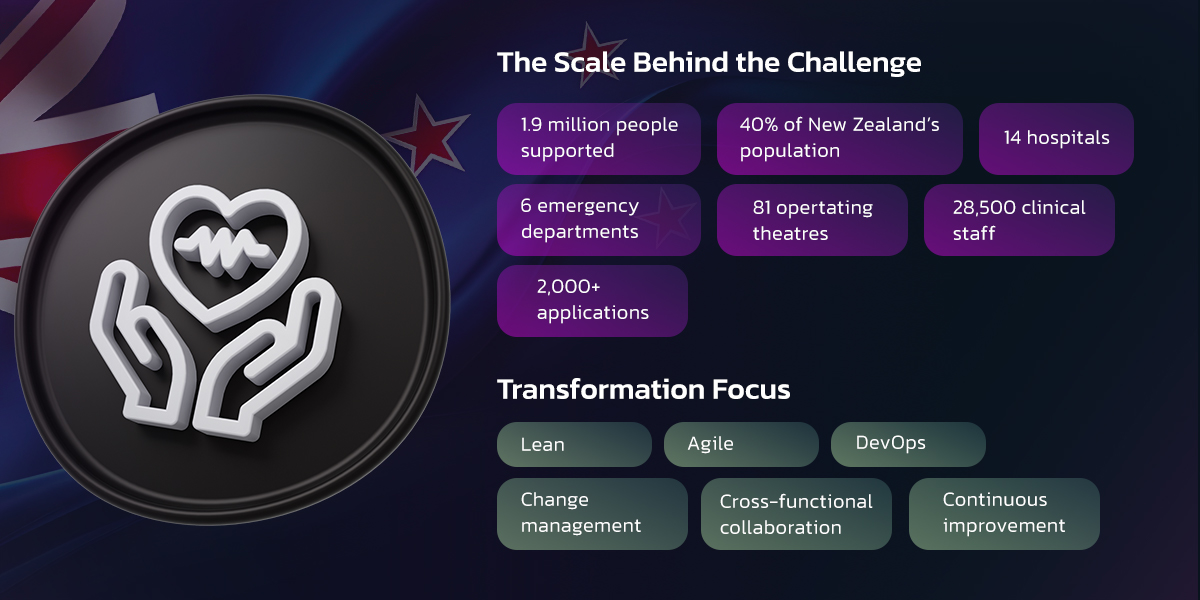
Citrus Global was brought in to partner with one of New Zealand's largest healthcare shared services organisations — a body responsible for the digital and operational infrastructure supporting nearly two million people across one of the most geographically expansive service areas in the Southern Hemisphere. The organisation at the centre of this engagement is responsible for healthcare shared services across nearly 20,000 square kilometres — a span of geographical coverage that would challenge even the most well-resourced logistics operation, let alone a technology and digital services function. It serves 1.9 million people. Close to 40% of an entire country’s population moves through the healthcare system it underpins.
The numbers inside that footprint are significant in their own right. Fourteen hospitals. Six emergency departments. Eighty-one operating theatres conducting more than 155,000 surgical procedures every year. Three thousand one hundred beds and 1.1 million bed-days annually. Twenty-eight thousand five hundred clinical staff whose ability to do their work — to care for patients, make decisions under pressure, and operate at the standard healthcare demands — depends, in part, on the reliability and responsiveness of the technology environment around them.
And that environment was being managed by a Digital and Mobility function responsible for more than 2,000 applications. More than two thousand distinct systems, integrated to varying degrees, each with its own change cycle, its own dependencies, and its own relationship to the clinical workflows it supported.
This was not an environment in which you could afford friction and simply absorb it later.
The Real Problem
The organisation was not struggling in any obvious sense. It was operational, capable, and staffed by experienced people who cared deeply about what they were delivering. But the operating model around them had not kept pace with what was now being asked of it. Delivery was still structured around traditional IT and business patterns, sequential, function by function, with long handoff chains between development, operations, and support. Feedback loops were slow. Change moved through layers of process that had been designed for control in a simpler environment, not for responsiveness in the one that now existed. The result was a widening gap between what the organisation needed to deliver and the speed and flexibility with which it could actually deliver it.
This was not fundamentally a technology problem. The real constraint sat in the operating model itself. In the beliefs, structures, habits, and cultural patterns governing how work moved through the organisation. And constraint at that level demands a very different kind of intervention than most technology engagements ever attempt.
Citrus Global understood that from the outset.
The Intervention
The transformation had three movements. Each one built on the last.
First, the mindset.
Before any framework was introduced, before any tool was configured, before any process was redesigned, Citrus Global worked with the organisation's teams at the level of belief — the assumptions people carried about how work should move, who owned what, and what good delivery actually looked like. The shift from sequential thinking to iterative thinking. From function-first to outcome-first. From "deliver, then inspect" to "build quality in, continuously."
This is the work that most transformation programmes skip because it is slower, less tangible, and harder to put in a progress report. It is also the reason most transformation programmes fail. You cannot introduce Agile mechanics into an organisation that has not shifted its underlying mental model, and expect anything other than Agile theatre. Citrus Global has seen that failure mode often enough that avoiding it is now structural to how they engage.
Second, Methods into real work.
With that foundation genuinely in place, Lean and Agile practices were introduced as a structured improvement applied directly to live work, with existing teams, under real delivery pressure. Iterative delivery cycles replaced sequential phases. Cross-functional collaboration replaced handoff-based coordination. Faster feedback loops connected the teams building and maintaining the platform to the clinical stakeholders whose operational needs were ultimately being served.
The Digital and Mobility function — responsible for managing the continuous, high-volume flow of change requests across 2,000+ applications — received particular focus. Structured agile tooling replaced ad hoc coordination. For the first time, the people doing the work had clarity about what was in the queue, what was in progress, what was blocked, and why. Stakeholders had visibility. Teams had the structural conditions to move with confidence
Third, the scale.
When early adoption within specific teams produced measurable results, Citrus Global extended the framework across major programmes standardising Lean-Agile and DevOps practices as the common operating language of the delivery function across the organisation. This is the inflection point where most transformation engagements fail. The pilot works. The team involved is energised. And then the organisation's immune system kicks in. The pressure to revert to familiar patterns.
Throughout all three movements, the engagement was not transactional. Citrus Global did not deliver a framework and disengage. They stayed, working alongside the organisation's teams through implementation, iteration, adjustment, and the long, unglamorous work of embedding change into daily practice until it became the natural way of operating rather than an additional effort on top of it.
The results are not soft. They are operational.

The outcomes that emerged from this engagement were operational, measurable, and lasting.
Delivery became faster and more predictable. Project timelines accelerated across the portfolio. Release cycles became reliable enough that the organisation could make commitments to clinical programmes — commitments that clinical teams plan real services around — with genuine confidence and follow through on them consistently. In a healthcare environment, that kind of predictability is not a performance metric. It is a quality-of-service obligation.
Structural collaboration replaced siloed coordination in a way that was genuinely observable. Development, operations, and support began working with shared accountability and shared visibility. The formal handoffs that had slowed everything down and obscured ownership gave way to cross-functional working patterns where teams understood the full arc of the work they were contributing to — not just their portion of it.
System reliability improved across the application portfolio. Better release discipline, stronger alignment between development and operations, more rigorous delivery practices, and the discipline of DevOps integration reduced downtime and improved stability across infrastructure that tens of thousands of clinical staff depend on every day.
And most significantly, the capability to keep improving remained after the engagement concluded. Lean thinking became embedded not as a programme but as a professional posture across the delivery function. The organisation developed genuine internal capacity to identify its own inefficiencies, run its own improvement cycles, and adapt to new pressures without needing an external trigger. That is the difference between an organisation that was transformed and one that can keep transforming. Citrus Global achieved both
What Endured
It was a fundamental redesign of how a critical public-sector organisation works — executed with precision, sustained with commitment, and built to last well beyond the engagement itself. The environment was high-stakes. The change required was cultural before it was technical. The execution was flawless in the ways that actually matter: the mindset shifted, the methods took hold, the scale was achieved, and the capability remained.
That is the standard Citrus Global operates at. It is the standard Cherry Global demands from every venture in the portfoli